Skip to content
Home
About Us
Our Locations
Board of Advisors
Code of Ethics
Before/After Care Fees
Calendar
Volunteer Opportunities
2027 Gala
Pre-Enrollment
Summer Camp Registration
Join Our Team
Contact Us
Search for...
Menu
Navigation Menu
Navigation Menu
Search for...
Home
About Us
Our Locations
Board of Advisors
Code of Ethics
Before/After Care Fees
Calendar
Volunteer Opportunities
2027 Gala
Pre-Enrollment
Summer Camp Registration
Join Our Team
Contact Us
Summer Camp Registration
Please enable JavaScript in your browser to complete this form.
Checkboxes (copy)
*
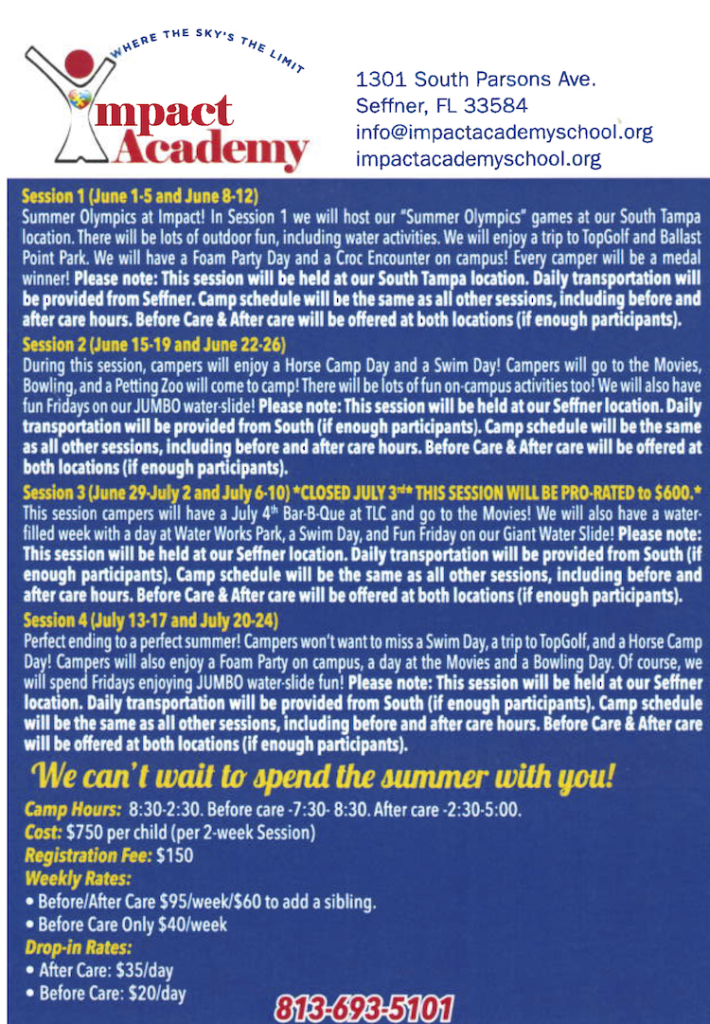
Session 1 – South Tampa – June 1, 2026 through June 12, 2026
Session 2 – Seffner – June 15, 2026 through June 26, 2026
Session 3 – Seffner – June 29, 2026 through July 10, 2026
Session 4 – Seffner – July 13, 2026 through July 24, 2026
Non-refundable registration fee of $150 is due at the time of registration. Camp cost is $750 per child per two week session. Campers must attend full sessions only. All summer camp fees MUST be paid two week prior to the beginning of the session(s) to be attended. Session 1 payment is due May 18, 2026. Session 2 payment is due June 1, 2026. Session 3 payment is due June 15, 2026. Session 4 payment is due June 29, 2026. All summer camp fees are non-refundable. Further information will be provided as it becomes available.
Email
*
Camper Name
*
First
Last
Has the camper previously attended Impact Academy's Summer Camp?
*
Yes
No
Parent Name(s)
*
Parent Occupation(s)
*
Address
*
Address Line 1
Address Line 2
City
— Select state —
Alabama
Alaska
Arizona
Arkansas
California
Colorado
Connecticut
Delaware
District of Columbia
Florida
Georgia
Hawaii
Idaho
Illinois
Indiana
Iowa
Kansas
Kentucky
Louisiana
Maine
Maryland
Massachusetts
Michigan
Minnesota
Mississippi
Missouri
Montana
Nebraska
Nevada
New Hampshire
New Jersey
New Mexico
New York
North Carolina
North Dakota
Ohio
Oklahoma
Oregon
Pennsylvania
Rhode Island
South Carolina
South Dakota
Tennessee
Texas
Utah
Vermont
Virginia
Washington
West Virginia
Wisconsin
Wyoming
State
Zip Code
DOB
*
MM
1
2
3
4
5
6
7
8
9
10
11
12
DD
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
YYYY
2027
2026
2025
2024
2023
2022
2021
2020
2019
2018
2017
2016
2015
2014
2013
2012
2011
2010
2009
2008
2007
2006
2005
2004
2003
2002
2001
2000
1999
1998
1997
1996
1995
1994
1993
1992
1991
1990
1989
1988
1987
1986
1985
1984
1983
1982
1981
1980
1979
1978
1977
1976
1975
1974
1973
1972
1971
1970
1969
1968
1967
1966
1965
1964
1963
1962
1961
1960
1959
1958
1957
1956
1955
1954
1953
1952
1951
1950
1949
1948
1947
1946
1945
1944
1943
1942
1941
1940
1939
1938
1937
1936
1935
1934
1933
1932
1931
1930
1929
1928
1927
1926
1925
1924
1923
1922
1921
1920
Diagnosis(es)
*
Primary Phone
*
Secondary Phone
Current School
*
Does student have: (Please check all that apply)
IEP
504 Plan
Please upload IEP/Behavior Plan
Drag & Drop Files,
Choose Files to Upload
You can upload up to 2 files.
Medical Insurance Company
*
Policy Number
ABA Therapy Company
*
Previously required 1/1?
*
Yes
No
Is your child potty-trained?
*
Yes
No
Does your child have a history of seizures?
*
Yes
No
Date of last seizure, if applicable.
Does your child have pica?
*
Yes
No
Is your child an elopement risk?
*
Yes
No
Does your child have allergies?
*
Yes
No
Allergies:
Does your child exhibit disruptive behavior?
*
Yes
No
Does your child take medicine during school hours?
*
Yes
No
List of current medications, if any.
Dietary Restrictions?
Additional Information?
Submit